Juliana Bonfleur Carvalho1, Jessica Madeira1, Carolina Ribeiro Correa1, Luis Rogerio Ferro Otaga1, Silmara Rodrigues Machado1, Natalia Golin1, Karina Kroth2, Erika Suiter1
1Hospital Sírio Libanês, São Paulo, SP, Brasil
2Nestle Health Science, São Paulo, SP, Brasil
Received: December 24, 2024; Accepted: January 13, 2025.
Correspondence: Juliana Bonfleur Carvalho, juliana.bcarvalho@hsl.org.br
How to cite
Carvalho JB, Madeira J, Correa CR, Otaga LRF, Machado SR, Golin N, Kroth K, Suiter E. Impact of Video-Based Nutritional Education on Dietary Habits of Elderly Duringthe COVID-19 Pandemic. Nutr Bras. 2024;23(5):1142-1153.doi:10.62827/nb.v23i5.3044
Abstract
Introduction: In March 2020, COVID-19 was declared a pandemic by the World Health Organization (WHO). Public health measures were adopted to curb the spread of the virus, that included guidelines for social isolation, with a particular emphasis on protecting vulnerable groups, such as the elderly. Throughout the pandemic, digital tools and internet browsing have served as powerful resources for overcoming social isolation, particularly among the elderly. Objective: To evaluate changes in the dietary habits of older individuals after receiving nutritional education via educational videos. Methods: A prospective, experimental community trial was conducted with women aged ≥60 years, who participated in a social project. In-person interviews, conducted at the project’s commencement and conclusion while adhering to safety protocols, were utilized for collecting clinical and anthropometric data. Additionally, a food frequency questionnaire, Mini Nutritional Assessment, and clinical frailty scale were administered. Monthly video lessons featuring educational content on nutrition, each not exceeding 10 minutes, were disseminated to the participants. Following the video lessons, an online forum was held, where a nutritionist addressed any questions regarding the content. Results: Twenty elderly women participated in the project, with a mean age (± standard deviation) of 68.6±6.9 years. Of the total, 45% (9) were obese, with a mean BMI of 35.7 kg/m2. Following the educational intervention, a significant improvement was observed in the consumption of vegetables and greens in soups (p=0.026). Furthermore, a significant reduction in the mean waist circumference was found (p=0.025). Conclusion: The initiative of promoting healthy eating through video lessons led to positive changes in the body composition and food consumption patterns of the elderly participants.
Keywords: Food and nutrition education; COVID-19; feeding behavior.
Resumo
Introdução: Em março de 2020, a COVID-19 foi declarada pandemia pela Organização Mundial da Saúde (OMS). Foram adotadas medidas de saúde pública para conter a propagação do vírus, que incluíram orientações para o isolamento social, com ênfase na proteção de grupos vulneráveis, como os idosos. Ao longo da pandemia, as ferramentas digitais e a navegação na Internet serviram como recursos poderosos para superar o isolamento social, especialmente entre os idosos. Objetivo: Avaliou-se mudanças nos hábitos alimentares de idosos após receberem educação nutricional por meio de vídeos educativos. Métodos: Realizou-se um ensaio comunitário prospectivo e experimental com mulheres com idade ≥60 anos, que participaram de um projeto social. Entrevistas presenciais, realizadas no início e na conclusão do projeto, respeitando os protocolos de segurança, foram utilizadas para a coleta de dados clínicos e antropométricos. Além disso, foram aplicados questionário de frequência alimentar, Mini Avaliação Nutricional e Escala de Fragilidade Clínica. Entre os encontros presenciais, foram divulgadas às participantes videoaulas mensais com conteúdos educativos sobre nutrição, cada uma com duração não superior a 10 minutos. Após as videoaulas, realizou-se um fórum online, onde uma nutricionista esclareceu eventuais dúvidas referentes ao conteúdo. Resultados: Participaram do projeto 20 idosas, com média de idade (± desvio padrão) de 68,6 ±6,9 anos. Do total, 45% (9) eram obesos, com IMC médio de 35,7 kg/m2. Após a intervenção educativa, observou-se melhora significativa no consumo de legumes e verduras em sopas (p=0,026). Além disso, foi encontrada redução significativa na média da circunferência da cintura (p=0,025). Conclusão: A iniciativa de promoção da alimentação saudável por meio de videoaulas proporcionou mudanças positivas na composição corporal e nos padrões de consumo alimentar dos idosos participantes.
Palavras-chave: Educação alimentar e nutricional; COVID-19; comportamento alimentar.
Introduction
The global population is rapidly aging. From 2000 to 2050, the proportion of the world’s population aged ≥60 years is projected to double, whereas the proportion of people aged ≥80 years is expected to nearly quadruple. Although this demographic shift represents a triumph in healthcare and socio-economic development, it also poses significant challenges to societies, due to the inconveniences that can accompany longer lifespans. Furthermore, significant inequalities among individuals, in their living conditions and socioeconomically persist both between and within continents and countries [1].
Planning and implementing health initiatives aimed at enhancing the quality of life for older individuals is imperative. One such initiative is developing strategies for healthy eating, which should be incorporated into the advice provided by healthcare professionals to the elderly and their families. These measures can help foster greater enjoyment, health, and safety in everyday meals [2]
In March 2020, COVID-19 was declared a pandemic by the World Health Organization (WHO). In response, various public health measures were adopted to curb the spread of the virus. [3] Notably, these measures included guidelines for social isolation, with a particular emphasis on protecting vulnerable groups, such as the elderly [4]
Throughout the pandemic, digital tools and internet browsing have served as powerful resources for overcoming social isolation, particularly among the elderly, who are increasingly using mobile technologies for health-related purposes. These tools have enabled continued social communication with relatives, friends, and work, despite physical distancing [5,6].
Furthermore, digital technologies can significantly contribute to health promotion and disease prevention. A key advantage of interventions via digital platforms is their potential for independent use at home, aligning seamlessly with constraints imposed by the pandemic [7].
The rising demand for digital health promotion technologies has underscored their role in addressing contemporary challenges faced by the elderly, particularly in endeavors aimed at lifestyle modifications and health condition improvement. This is achieved through the delivery of health education materials grounded in science and presented in easily understandable language [8].
In this context, the present study implemented distance learning strategies for elderly participants in a social project. It provided nutritional education focused on healthy eating through digital platforms. The aim was to offer guidance on adopting healthy habits and suitable dietary choices for this age group during the challenging period of the pandemic.
Methods
This was a prospective, experimental community trial, designed to describe the experiences of food and nutrition education initiatives within a social project in São Paulo during the COVID-19 pandemic. There are 50 people participating in the social project (46 women and 4 men). The nutrition education project was presented to everyone and 20 women were interested and willing to participate. The study did not require a sample size calculation, as it included all 20 elderly women who wants participated from October 2022 to March 2023. Thus, it encompassed the entire tangible universe for the estimation of the parameters under study.
Following were the exclusion criteria: (i) refusal to participate; (ii) inability to participate in the initial face-to-face meeting; and/or (iii) inability to access the monthly videos due to lack of internet connectivity.
The study was submitted to the Research Ethics Committee (REC) of the institution. Number: 66370822.3.0000.5461
Research Procedures
The study was conducted by 3 previously trained nutritionists and carried out in three stages (Figure 1).
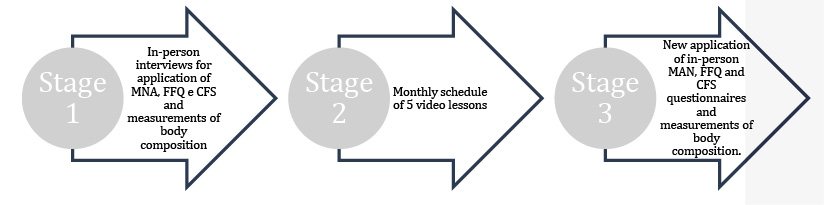
Figure 1 - Study flowchart
The first stage was face-to-face interviews, consisting of individual interviews with one nutritionist per participant and an interval of 1 hour each. After agreeing to participate in the study and signing the Informed Consent Form, the elderly women underwent the Mini Nutritional Assessment (MNA); furthermore, they were made to answer a Food Frequency Questionnaire (FFQ) adapted from the National Health Agency - Ministry of Health of Brazil, and the culturally adapted Portuguese version of the Clinical Frailty Scale [9,10]. The FFQ questionnaire was adapted from Vigitel, 2014 and consisted of a questionnaire with options for the frequency of weekly and daily consumption of 11 foods that covered the food groups.
Next, they underwent the assessments for body composition. Anthropometric measurement errors are reduced when carried out by the same professionals. Aiming to reduce inter and intra-evaluator measurement errors the nutritionists received training to have anthropometric measurements. It consisted of defining an adequate time interval between measurements (non-consecutive) and accurately marking the anatomical points. The body measurements taken were:
- Weight: measured with the elderly positioned centrally on an Omron HBF-514® (Omron, Kyoto, Japan) scale, standing upright, barefoot, in light clothing, with weight evenly distributed on both feet.
- Height: measured with the elderly barefoot, without headgear, standing against a wall in an anatomical position. The calf, buttocks, shoulders, and head were in contact with the wall, facing forward, and aligned with the Frankfurt Plane.
- Body Mass Index (BMI): calculated by dividing weight (kg) by the square of height (m). It is classified based on the cutoff points recommended by the Pan American Health Organization (PAHO) [11] as follows: underweight (BMI<23 kg/m2), normal weight (23≤BMI<28 kg/m2), overweight (28≤BMI<30 kg/m2), and obese (BMI≥30 kg/m2);
- Arm circumference (AC): measured at the midpoint between the acromial process and the end of the olecranon using an inelastic tape measure, ensuring the tape is snug but not compressing the skin. It is classified according to the percentage of adequacy as proposed by Blackburn and Thomton, 1979 [12];
- Triceps skinfold thickness (TSF): measured on the posterior aspect of the arm, parallel to the longitudinal axis, at the midpoint between the acromion and the olecranon, using a Sany AD1009C® (Sany, São Paulo, Brazil) caliper. It is classified according to the percentage of adequacy as proposed by Blackburn and Thomton, 1979 [12];
- Arm muscle circumference (AMC): calculated from the values of AC and TSF using the equation: The classification is based on the percentile values proposed by Frisancho (1990) [13];
- Waist circumference (WC): measured at the midpoint between the last rib and the iliac crest using a tape measure. It is classified as a predictor of cardiovascular risk with values ≥ 94 cm for men and ≥ 80 cm for women. Values of ≥ 102 cm for men and ≥ 88 cm for women are considered to indicate a very high risk, according to the 1998 WHO guidelines (13) [14];
- Calf circumference (CC): measured at the most protruding portion of the calf using a tape measure. A calf circumference of <34 cm for men and <33 cm for women is considered indicative of reduced muscle mass [15].
In the second stage, video lessons were provided to the elderly on a monthly schedule.
The video lessons theme, each lasting a minimum of 6 minutes and a maximum of 10 minutes, were:
- Healthy eating
- Hydration
- Conscious sodium intake
- Relationship between food and memory
- Proper protein consumption
They were created using software such as Windows Media Player® (Microsoft, Redmond, Washington, USA) and Inshot (Dún Laoghaire, Dublin, Ireland). The content was distributed through a free communication app, accessible on personal devices such as cell phones and computers.
Alongside the release of each video lesson, a dedicated forum was established, using the same app in which the videos were made available. In this forum, a nutritionist was available to address any questions related to the topics covered in the classes.
In the third stage, the data obtained from the first interview were reassessed. Additionally, a satisfaction survey was conducted by a trained administrative employee in an isolated environment to prevent influencing the participants’ answers.
Statistical analysis
Statistical analysis was performed using summary measures, including mean, standard deviation, absolute and relative frequencies (percentage), as well as bar graphs and boxplots.
The following inferential analyses were used to confirm or reject hypotheses based on the evidence revealed in the descriptive analysis:
- Student’s t-test was employed for dependent samples [16] to compare numerical variables with normal distributions across two time periods.
- Wilcoxon test [17] was employed to compare numerical variables that did not follow a normal distribution across two time periods.
- McNemar test [18] was used to compare binary categorized variables across two time periods.
An alpha significance level of 5% was set for all conclusions derived from inferential analyses. Data entry was performed in Excel (Microsoft) spreadsheets to ensure proper storage and management of the information. Statistical analyses were conducted using IBM SPSS Statistics software, version 24, and R, version 3.6.3 [19].
Results
Initially, 20 elderly women were evaluated, with an average age (± standard deviation [SD]) of 68.6±6.9 years. Common comorbidities were observed, with 75% (15) having hypertension, 30% (6) diabetes, 10% (2) cancer, and 5% (1) cardiovascular disease.
The results of malnutrition risk screening, assessed by the MNA, revealed that 67% participants had a normal nutritional status before the interventions, and this increased to 83% after the interventions (p=0.687).
Regarding BMI, 45% (9) of the participants were classified as obese with a mean BMI of 35.7 kg/m², 25% (5) as overweight (mean BMI of 28.3 kg/m²), 20% (4) as normal weight (mean BMI of 24 kg/m²), and 10% (2) as underweight (mean BMI of 21.3 kg/m²). The CFS assessment revealed that 60% (12) of participants were active, 20% (4) were moderately active, 15% (3) were highly active, and 5% (1) were vulnerable. Table 1 presents food consumption data according to the FFQ.
Table 1 - Food Frequency of the Elderly Participants in the Social Project (October 2022–March 2023)
|
Food frequency |
||||||||||||
|
Food |
1–2 days/week |
3–4 days/week |
5–6 days/week |
Every |
Almost Never |
Never |
||||||
|
n |
% |
n |
% |
n |
% |
n |
% |
n |
% |
n |
% |
|
|
Beans |
3 |
15 |
5 |
25 |
2 |
10 |
6 |
30 |
2 |
10 |
2 |
10 |
|
Raw Vegetables |
2 |
10 |
3 |
15 |
0 |
0 |
12 |
60 |
1 |
5 |
0 |
0 |
|
Cooked Vegetables |
0 |
0 |
9 |
45 |
4 |
20 |
7 |
35 |
0 |
0 |
0 |
0 |
|
Vegetables in Soups |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
Meat |
9 |
45 |
5 |
25 |
1 |
5 |
2 |
10 |
1 |
5 |
2 |
10 |
|
Chicken |
7 |
35 |
6 |
30 |
4 |
20 |
1 |
5 |
1 |
5 |
1 |
5 |
|
Fresh Fruit Juice |
2 |
10 |
0 |
0 |
1 |
5 |
9 |
45 |
5 |
25 |
3 |
15 |
|
Fruit |
4 |
20 |
2 |
10 |
0 |
0 |
13 |
65 |
1 |
5 |
0 |
0 |
|
Soda/Artificial Juice |
5 |
25 |
0 |
0 |
1 |
5 |
0 |
0 |
6 |
30 |
8 |
40 |
|
Milk |
6 |
30 |
2 |
10 |
2 |
10 |
6 |
30 |
2 |
10 |
2 |
10 |
|
Sweets |
6 |
30 |
1 |
5 |
1 |
5 |
3 |
15 |
8 |
40 |
1 |
5 |
|
Replace lunch |
1 |
5 |
1 |
5 |
1 |
5 |
2 |
10 |
3 |
15 |
12 |
60 |
|
Replace dinner |
3 |
15 |
1 |
5 |
0 |
0 |
5 |
25 |
5 |
25 |
6 |
30 |
|
Alcoholic beverages |
2 |
10 |
1 |
5 |
0 |
0 |
0 |
0 |
7 |
35 |
10 |
50 |
After the second stage of the study, involving video lessons with educational content, a significant change was observed in the consumption of vegetables in soups (p=0.026) compared to that in the first stage, as illustrated in the figure below.
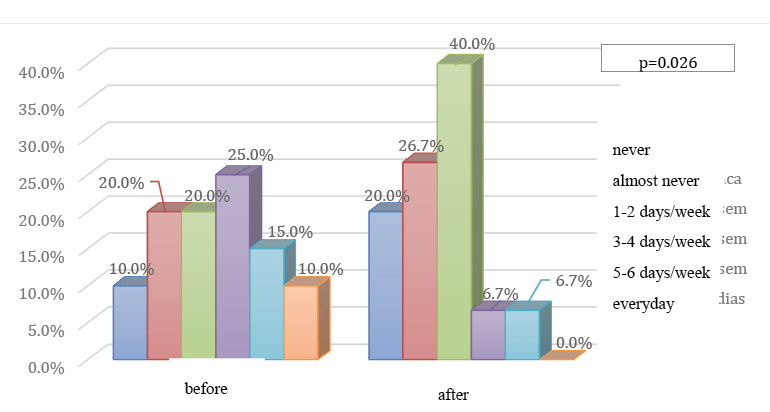
Figure 2 - Consumption of Vegetables in Soups among Elderly participants in the Social Project (October 2022–March 2023) * p <0.05
Six months after the first evaluation, 15 elderly women participated in the third stage of the study. Table 2 presents the anthropometric assessment at both the beginning and end of the project.
Table 2 - Anthropometric Assessment of the Elderly Participants in the Social Project (October 2022 –March 2023)
|
Initial Assessment |
Second Assessment |
p-value |
|
|
Mean (SD) |
Mean (SD) |
||
|
Arm Circumference (AC; cm) |
31.60 (7.75) |
32.73 (5.05) |
0.955a |
|
Triceps Skinfold Thickness (TSF; mm) |
25.98 (7.64) |
23.75 (6.81) |
0.485b |
|
Calf Circumference (Adjusted CC; cm) |
33.73 (2.71) |
34.88 (3.88) |
0.143b |
a Wilcoxon test, b Student’s t-test for dependent samples
A statistically significant reduction was observed in the mean waist circumference of the participants after the interventions, as illustrated in Figure 3.
Before
Waist circunference (cm)
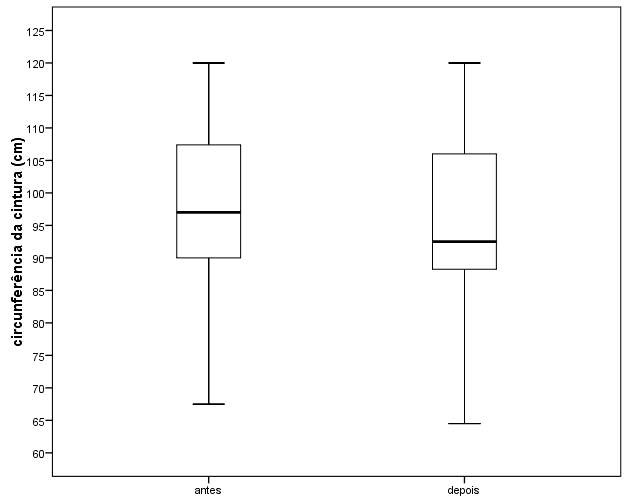
* Statistically significant (p<0.05).
Figure 3 - Comparison of the participants’ waist circumference at project commencement and post-interventions
About satisfaction survey, the main complaints regarding the methodology were familiarity with cell phone use, audio adequacy and internet network connection failure at times.
Discussion
Conducting follow-ups with the elderly during the COVID-19 pandemic posed multifaceted challenges, particularly in fostering healthy eating habits amidst the difficulties of the period. Many elderly were isolated for extended periods, necessitating adaptations to novel forms of communication and self-care. The older individuals often encounter obstacles to adequate food intake, such as reduced physical function, financial constraints, and chewing difficulties, among others. However, limited evidence exists regarding the types of support and strategies that prove effective for older adults in maintaining their nutritional status, especially during the COVID-19 pandemic [20].
Initially, the study evaluated 20 elderly women already engaged in a community program for the older individuals. The withdrawal of some participants during the course of the study can be attributed to the challenges faced by certain elderly people in using electronic media. This usage was one of the requirements for participation due to social distancing measures.
Women represented 100% of the study population, indicating a potentially higher level of health consciousness among the female participants. Additionally, the study by Capicio et al, 2022, also highlights gender differences observed in social isolation behavior, with women tending to remain more isolated than men [20].
Regarding body mass index, 70% (14) were obese or overweight. The changes in body composition associated with aging are characterized by a decrease in muscle mass and an increase in adipose tissue. This alteration is more pronounced in women, who also experience significant hormonal changes as they age [21,22]. After the interventions, a reduction in the average BMI from 30.1 kg/m2 to 29.0 kg/m2 was observed, although this change was not statistically significant.
In our evaluation of the eating frequency among the elderly participants (Table 1), we found that 25% (5) reported almost never consuming natural juices, another 25% (5) consumed soft drinks or artificial juices 1 to 2 times per week, and a further 25% (5) replaced dinner with snacks every day. This pattern may be attributed to the difficulties faced by the elderly in cooking, compounded by a lack of motivation stemming from loneliness during meals. Moreover, the isolation during the pandemic may have exacerbated this situation. Another challenge relates to the difficulty in acquiring fresh foods, such as fruits, during social isolation [23]. Classes on healthy eating and hydration provided the elderly with practical and feasible ways to enhance their food consumption while still maintaining their usual habits. Examples include healthy snacks containing carbohydrates, high-quality fats, and proteins, as well as flavored waters that are quick and easy to prepare, offering a healthier alternative to artificial soft drinks and juices.
As seen in Figure 1, a statistically significant increase was observed in vegetable consumption in soups among the participants, while methods such as boiling or grilling did not exhibit a similar increase. This is likely due to the elderly’s preference for softer foods, as they often face challenges with chewing. Consequently, this led to a positive increase in the consumption of vitamins and minerals, which are crucial for the elderly. These findings aligned with those of the systematic review by Teggart K, et al. (2022), which indicated that five studies noted improvements in certain aspects of food and fluid intake, but not all, following nutritional education [24].
The older individuals are accustomed to certain dietary routines, which hinders the process of change and necessitates the enhancement of tailored nutritional education strategies for this demographic. In the present study, nutritional interventions were conducted in groups, providing access to a professional nutritionist online to address any questions raised following the viewing of healthy eating video lessons. This approach facilitated interactive discussions, highlighting the benefits of assisting the elderly in learning from each other’s knowledge and experiences, and consequently, in overcoming environmental barriers to healthy eating.
A statistically significant reduction was observed in the average waist circumference of the participants after six months of intervention. This outcome is advantageous for the elderly women in the program, as the reduction in abdominal fat indicates a reduction in visceral fat. The accumulation of visceral fat is known to increase the risk of developing cardiovascular diseases, cancer, diabetes, and other metabolic disorders. This risk is further heightened in postmenopausal women [25]. The 100% prevalence of comorbidities among participants in this study underscores the importance of implementing measures aimed at improving these conditions.
In addition to reducing fat, increasing muscle mass has positive impacts on the health of the elderly. The measurement of the calf circumference serves as a direct indicator of muscle mass. Although not statistically significant, an increase was observed in calf circumference post-interventions, as shown in Table 2. Adequate protein intake is associated with the maintenance and recovery of muscle mass, especially when combined with physical activity [26,27]. During the educational intervention, the elderly participants were provided video lessons that demonstrated the importance and practical ways of incorporating protein into their diets. Maintain a normal lean body mass is generally associated with better overall health, including the prevention of muscle weakness and reduced functional declines associated with aging [26].
In the frailty assessment, muscle weakness was considered as one of the phenotypes [27]. Only 5% (1) of the elderly participants were classified as vulnerable, which can likely be attributed to the following reasons. Firstly, they had adequate average muscle mass (33.7 cm) at the beginning of the study and were actively participating in a community support group. Secondly, their active participation in the group provided continuous guidance and follow-up for regular physical activity. Additionally, before the pandemic, they received support from a multidisciplinary team consisting of a psychologist, nutritionist, physical educator, and dentist. Even during the pandemic, they continued to receive remote support from these professionals.
The presence of community programs specifically tailored for the older individuals are crucial, as they address their specific nutritional needs and facilitate adaptation to the changes inherent to aging. The complex interplay of financial, psychosocial, environmental, physical, cognitive, gender, and cultural factors is known to influence eating behavior, food access, and mobility [24].
As a limitation, the current study may have been subject to bias because the participants were elderly individuals already enrolled in a community program offering physical activity classes and nutritional counseling before the pandemic. This prior enrollment could imply better health conditions, including nutritional, functional, and cognitive status. We have to consider that as the intervention was carried out remotely during the Pandemic, the results may have been influenced by external factors such as the eating habits of other people who lived with the elderly, emotional factors or information received through other means of communication.
Conclusion
The promotion of healthy eating through video lessons led to positive changes in body composition and dietary habits among the elderly women who had previously received multidisciplinary care before the onset of the COVID-19 pandemic.
Conflict of interest
The authors report no conflicts of interest.
Financing source
None.
Authors’ contributions
Conception and design of the research: Suiter E, Madeira J, Otaga LR, Golin N, Carvalho JB, Kroth K, Correa CR; Data collection: Madeira J, Otaga LR, Golin N, Correa CR, Kroth K; Data analysis and interpretation: Madeira J, Otaga LR, Golin N, Carvalho JB, Kroth K; Statistical analysis: Madeira J; Otaga LR, Santos G; Manuscript writing: Madeira J, Otaga LR, Golin N, Carvalho JB, Kroth K, Correa CR; Critical revision of the manuscript for important intellectual content: Suiter E, Madeira J, Otaga LR, Golin N, Carvalho JB, Kroth K, Correa CR, Machado SR.
References
1. Bautmans I, Knoop V, Thiyagarajan JA, et al. WHO working definition of vitality capacity for healthy longevity monitoring. Lancet Healthy Longev. 2022;3:e789-e796. doi:10.1016/S2666-7568(22)00200-8.
2. Daniela MS, Dewelyn DA, Estefânia FSP. Food and nutrition education actions with the elderly in times of pandemic: Impacts and challenges. Braz J Health Rev. 2021;4:13961-72. Available from: https://ojs.brazilianjournals.com.br/ojs/index.php/BJHR/article/view/31826.
3. Allan M, Lièvre M, Laurenson-Schafer H, et al. The World Health Organization COVID-19 surveillance database. Int J Equity Health. 2022;21 Suppl 3:167. doi:10.1186/s12939-022-01767-5.
4. Sepúlveda-Loyola W, Rodríguez-Sánchez I, Pérez-Rodríguez P, et al. Impact of social isolation due to COVID-19 on health in older people: Mental and physical effects and recommendations. J Nutr Health Aging. 2020;24:938-47. doi:10.1007/s12603-020-1469-2.
5. Cilli E, Ranieri J, Guerra F, Colicchia S, Di Giacomo D. Digital affinity and cognitive reserve: Salience for resilient aging in pandemic. Gerontol Geriatr Med. 2023;9:23337214231162773. doi:10.1177/23337214231162773.
6. Banskota S, Healy M, Goldberg EM. 15 smartphone apps for older adults to use while in isolation during the COVID-19 pandemic. West J Emerg Med. 2020;21:514-25. doi:10.5811/westjem.2020.4.47372.
7. De Santis KK, Mergenthal L, Christianson L, et al. Digital technologies for health promotion and disease prevention in older people: Scoping review. J Med Internet Res. 2023;25:e43542. doi:10.2196/43542.
8. Krishnaswami A, Beavers C, Dorsch MP, et al. Gerotechnology for older adults with cardiovascular diseases: JACC state-of-the-art review. J Am Coll Cardiol. 2020;76:2650-70. doi:10.1016/j.jacc.2020.09.606.
9. Rodrigues MK, Nunes Rodrigues I, Vasconcelos Gomes da Silva DJ, de S Pinto JM, Oliveira MF. Clinical frailty scale: Translation and cultural adaptation into the Brazilian Portuguese language. J Frailty Aging. 2021;10:38-43. doi:10.14283/jfa.2020.7.
10. Brasil. Ministério da Saúde. Vigitel Brasil 2014 Saúde Suplementar: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Brasília: Ministério da Saúde; 2015. Available from: https://bvsms.saude.gov.br/bvs/publicacoes/vigitel_brasil_2014.pdf.
11. Organización Panamericana de la Salud. Encuesta Multicentrica salud bienestar & envejecimiento (SABE) en América Latina y el Caribe: Informe Preliminar. Washington, DC: OPS; 2001. Available from: http://www.opas.org/program/sabe.html.
12. Blackburn GL, Thornton PA. Nutritional assessment of the hospitalized patients. Med Clin North Am. 1979;63:1103-11. Available from: https://pubmed.ncbi.nlm.nih.gov/116095/.
13. Frisancho AR. Anthropometric standards for the assessment of growth and nutritional status. Ann Arbor: University of Michigan Press; 1990. Available from: https://press.umich.edu/Books/A/Anthropometric-Standards-for-the-Assessment-of-Growth-and-Nutritional-Status.
14. World Health Organization (WHO). Physical status: The use and interpretation of anthropometry. Geneva: WHO; 1998. Available from: http://apps.who.int/iris/bitstream/10665/37003/1/WHO_TRS_854.pdf.
15. Barbosa-Silva TG, Bielemann RM, Gonzalez MC, Menezes AM. Prevalence of sarcopenia among community-dwelling elderly of a medium-sized South American city: Results of the COMO VAI? study. J Cachexia Sarcopenia Muscle. 2016;7:136-43. doi:10.1002/jcsm.12049.
16. Bussab WO, Morettin PA. Estatística básica. 5ª ed. São Paulo: Saraiva; 2006.
17. Siegel S. Estatística não-paramétrica para ciências do comportamento. 2ª ed. Porto Alegre: Artmed; 2006.
18. Agresti A. Categorical data analysis. New York: Wiley Interscience; 1990.
19. R Core Team. R: A language and environment for statistical computing. Vienna: R Foundation for Statistical Computing; 2016. Available from: http://www.R-project.org/.
20. Capicio M, Panesar S, Keller H, et al. Nutrition risk, resilience and effects of a brief education intervention among community-dwelling older adults during the COVID-19 pandemic in Alberta, Canada. Nutrients. 2022;14:1110. doi:10.3390/nu14051110.
21. Ko SH, Jung Y. Energy metabolism changes and dysregulated lipid metabolism in postmenopausal women. Nutrients. 2021;13:4556. doi:10.3390/nu13124556.
22. Paranhos Amorim DN, Nascimento DDC, Stone W, Alves VP, Coelho Vilaça E Silva KH. Body composition and functional performance of older adults. Osteoporos Sarcopenia. 2022;8:86-91. doi:10.1016/j.afos.2022.04.002.
23. Ellis A, Jung SE, Palmer F, Shahan M. Individual and interpersonal factors affecting dietary intake of community-dwelling older adults during the COVID-19 pandemic. Public Health Nutr. 2022;25:1-29. doi:10.1017/S1368980022000696.
24. Teggart K, Ganann R, Sihota D, et al. Group-based nutrition interventions to promote healthy eating and mobility in community-dwelling older adults: A systematic review. Public Health Nutr. 2022;25:2920-51. doi:10.1017/S136898002200115X.
25. Silveira EA, Kliemann N, Noll M, Sarrafzadegan N, de Oliveira C. Visceral obesity and incident cancer and cardiovascular disease: An integrative review of the epidemiological evidence. Obes Rev. 2021;22:e13088. doi:10.1111/obr.13088.
26. Putra C, Konow N, Gage M, York CG, Mangano KM. Protein source and muscle health in older adults: A literature review. Nutrients. 2021;13:743. doi:10.3390/nu13030743.
27. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: Evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:M146-M156. doi:10.1093/gerona/56.3.m146.
