doi: 10.62827/fb.v27i2.1152
Aquatic physical therapy reduces pain, improves functional fitness and quality of life of older people with knee osteoarthritis: Randomized controlled trial
A fisioterapia aquática reduz a dor, melhora a aptidão funcional e qualidade de vida de idosos com osteoartrite de joelho: Ensaio clínico randomizado
Guilherme Eleutério Alcalde1, Bruna Pianna2, Thais Fernanda Bôscoa Gallassi3, Karina Graziela Paccola Alcalde2, Fabio Alexandre Casarin Pastor1, Manuelly Francine Lopes1, Maria Giulia Eguea Chiachio1, Eduardo Aguilar Arca4
1Universidade do Oeste Paulista (UNOESTE), Jaú, SP, Brasil
2Universidade Estadual Paulista (UNESP), São Paulo, SP, Brasil
3Associação Educacional do Vale da Jurumirim (UNEDUVALE), Avaré, SP, Brasil
4Centro Universitário Sagrado Coração (UNISAGRADO), Bauru, SP, Brasil
Received: December 16, 2025; Accepted: March 2, 2026.
Correspondence: Guilherme Eleutério Alcalde, guilhermealcalde@unoeste.br
How to cite
Alcalde GE, Pianna B, Gallassi TFB, Alcalde KGP, Pastor FAC, Lopes MF, Chiacio MGE, Arca EA. Aquatic physical therapy reduces pain, improves functional fitness and quality of life of older people with knee osteoarthritis: randomized controlled trial. Fisioter Bras. 2026;27(2):3062-3072 doi: 10.62827/fb.v27i2.1152.
Abstract
Introduction: Aquatic therapy promotes short-term benefits for patients with knee osteoarthritis, the first therapeutic option for the elderly with this pathological condition. Objective: Investigate the effects of an aquatic physical therapy program on pain intensity, functional fitness and quality of life in older people with knee osteoarthritis. Methods: This was a two-arm parallel randomized controlled clinical trial with older people with knee osteoarthritis. The volunteers were divided into: water group (WG; n = 18), who were subjected to the intervention, and control group (CG; n = 15), who were not subjected to any kind of intervention. Data collection consisted of the evaluation of the perception of pain by visual analog scale with application of nociceptive stimuli at four anatomical points of the knee, functional fitness tests, and application of the WHOQOL-bref and WOMAC questionnaires, pre- and post-intervention. The program lasted 12 weeks, periodicity of three times a week, 40 minutes per session, water temperature maintained at 33o C and consisted of aerobic and functional exercises in the form of circuit training. Results: There was a reduction in pain intensity in the articular interline and medial femoral condoyle of the left knee, increased flexibility, improvement in the dynamic balance, pain and physical function domains of WOMAC and environmental domain of WHOQOL-bref. Conclusion: We conclude that the aquatic physical therapy promoted reduction of pain intensity, improved functional fitness and quality of life in older people with knee osteoarthritis.
Keywords: Hydrotherapy; Chronic Pain; Range of Motion.
Resumo
Introdução: A terapia aquática promove benefícios em curto prazo para pacientes com osteoartrite de joelho, sendo uma das primeiras opções terapêuticas para idosos com essa condição patológica. Objetivo: Investigar os efeitos de um programa de fisioterapia aquática sobre a intensidade da dor, a aptidão funcional e a qualidade de vida em idosos com osteoartrite de joelho. Métodos: Trata-se de um ensaio clínico randomizado, controlado, de dois braços paralelos, realizado com idosos com osteoartrite de joelho. Os voluntários foram divididos em: grupo água (GA; n = 18), submetido à intervenção, e grupo controle (GC; n = 15), que não recebeu nenhum tipo de intervenção. A coleta de dados consistiu na avaliação da percepção da dor por meio da escala visual analógica, com aplicação de estímulos nociceptivos em quatro pontos anatômicos do joelho, realização de testes de aptidão funcional e aplicação dos questionários WHOQOL-bref e WOMAC, antes e após a intervenção. O programa teve duração de 12 semanas, com frequência de três vezes por semana, 40 minutos por sessão, temperatura da água mantida a 33°C, e consistiu em exercícios aeróbicos e funcionais em formato de circuito. Resultados: Observou-se redução da intensidade da dor na interlinha articular e no côndilo femoral medial do joelho esquerdo, aumento da flexibilidade, melhora do equilíbrio dinâmico, bem como melhora nos domínios dor e função física do WOMAC e no domínio meio ambiente do WHOQOL-bref. Conclusão: Conclui-se que a fisioterapia aquática promoveu redução da intensidade da dor, melhora da aptidão funcional e da qualidade de vida em idosos com osteoartrite de joelho.
Palavras-chave: Hidroterapia; Dor Crônica; Amplitude de Movimento Articular.
Introduction
Knee osteoarthritis (OA) is a chronic and degenerative rheumatic disease, common in the elderly and which presents a reduction in the articular space, osteophytes, subchondral bone sclerosis and deformity of the bone contour [1,2].
Aquatic therapy can be considered the first therapeutic option for older adults with knee OA, as the immersion exercises performed promote multidimensional resistance with minimal overload on the joints, helping to reduce pain, increase flexibility, improve dynamic balance and quality of life (QL) [3,4].
Based on these assumptions the following hypothesis was formulated: “Aquatic physical therapy programs contribute to an increased pain threshold, improved functional fitness and quality of life in older adults with knee OA.” The objective of the study was to verify the effects of an aquatic physical therapy program on the perception of pain, functional fitness and quality of life in older people with knee OA.
Methods
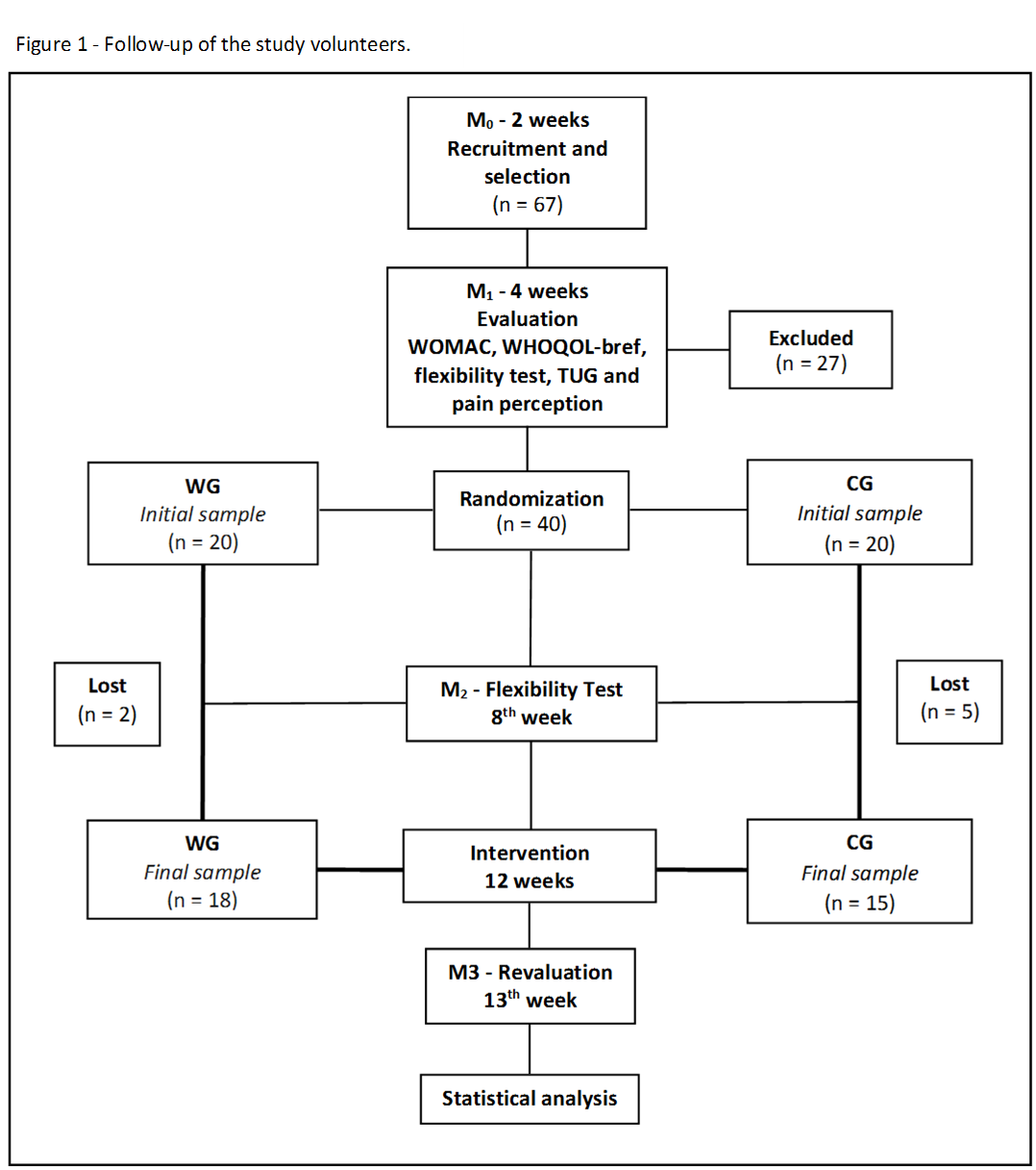
This study consisted of a two-arm parallel randomized controlled therapeutic clinical trial involving elderly volunteers diagnosed with knee osteoarthritis. The project was approved by the Research Ethics Committee of the Universidade do Sagrado Coração (approval number 1,131,248), and all participants signed the Free and Informed Consent Form prior to data collection. The study protocol was registered in the Brazilian Registry of Clinical Trials (ReBec) under registration number RBR-78h48d. Data collection was carried out at the Physical Therapy Research Laboratory, and the intervention program took place at the Therapeutic Pools Laboratory of the Universidade do Sagrado Coração, in Bauru, São Paulo, Brazil. Elderly individuals of both sexes with unilateral and/or bilateral knee osteoarthritis classified as moderate, severe, or very severe according to Lequesne’s algofunctional questionnaire were included. Exclusion criteria comprised unstable heart conditions, inability to ambulate, knee or hip arthroplasty, epilepsy, fibromyalgia, or any contraindication to aquatic therapy. Sample size calculation was performed using the G*Power software, considering an alpha level of 5% and a beta of 80%, resulting in 15 participants per group, with pain intensity used as the primary variable for calculation. A total of 67 individuals were screened, and 27 were excluded. The random allocation of the 40 eligible participants was performed using The Hat®️ 3.0.2 software, and they were divided into a water group (WG; n = 20), which underwent the intervention, and a control group (CG; n = 20), which did not receive any intervention. The evaluative instruments included the WHOQOL-BREF questionnaire, composed of 26 questions distributed across physical, psychological, social, and environmental domains, and the WOMAC questionnaire, a specific instrument for knee osteoarthritis divided into three domains: pain (5 items), joint stiffness (2 items), and physical function (17 items), scored using a Likert scale ranging from 0 to 100 points. Pain perception was assessed using a dolorimeter (Palpeter®️) with 1 kg precision, applying pressure to four predefined anatomical points of the knee, followed by pain measurement using the Visual Analog Scale (VAS). Functional mobility was evaluated using the Timed Up and Go (TUG) test, and flexibility was assessed using the sit-and-reach test; both were performed three times, and the best performance was recorded. The aquatic therapy program lasted 12 weeks, with three 40-minute sessions per week, and water temperature maintained at 33°C. The study design was structured into four stages: M0 – recruitment and selection (two weeks); M1 – baseline evaluation (four weeks); M2 – intermediate reassessment with the sit-and-reach test (eighth week); and M3 – revaluation (thirteenth week), as shown in Figure 1.
Prepared by the authors (2026).
Data normality was verified with the Shapiro-Wilk test. Parametric data were expressed as mean and standard deviation, by using the Student’s t-test for independent samples to compare groups and paired samples to compare the moments. For the analysis of repeated measures ANOVA was used with post-hoc Tukey. Nonparametric data were expressed as median, maximum and minimum values. To compare the groups we used the Mann-Whitney test and for comparison of moments the Wilcoxon test was used. In all tests, a result was considered statistically significant when p < 0.05.
Results
The baseline characteristics of the participants in both groups are presented in Table 1.
|
WG (n = 20) |
CG (n = 20) |
|
|
Age (years) |
66.11 ± 4.43 |
63.53 ± 6.26 |
|
Gender (M / F) |
13F/7M |
15F/5M |
|
Anthropometry |
||
|
Body weight (kg) |
77.06 ± 15.79 |
76.49 ± 18.16 |
|
Height (cm) |
1.62 ± 0.09 |
1.58 ± 0.09 |
|
BMI (kg / m2) |
29.19 ± 4.38 |
30.16 ± 5.99 |
|
AC (cm) |
98.00 ± 13.07 |
101.20 ± 13.37 |
|
Blood pressure |
||
|
SBP (mmHg) |
134.00 ± 23.48 |
135.00 ± 23.95 |
|
DBP (mmHg) |
86.00 ± 17.59 |
85.00 ± 16.70 |
|
Osteoarthritis diagnosis |
||
|
Right knee |
7 (35%) |
6 (30%) |
|
Left knee |
4 (20%) |
5 (25%) |
|
Bilateral |
9 (45%) |
9 (45%) |
|
Lequesne Questionnaire |
||
|
Very serious |
3 (15%) |
9 (45%) |
|
Serious |
14 (70%) |
8 (40%) |
|
Moderate |
3 (15%) |
3 (15%) |
|
Reported comorbidity |
||
|
Arterial hypertension |
14 |
10 |
|
Diabetes mellitus |
5 |
4 |
|
Others |
- |
- |
|
Medication |
||
|
Antihypertensives |
14 |
10 |
|
Antidiabetics |
5 |
4 |
|
Analgesics |
5 |
5 |
|
Anti-inflammatories |
2 |
1 |
|
Chondroprotectives |
11 |
10 |
WG: Water Group; CG: Control Group. Data presented as mean and standard deviation. BMI: body mass index; AC: abdominal circumference; SBP: systolic blood pressure; DBP: diastolic blood pressure. p> 0.05 for all comparisons.
Changes in quality of life domains assessed by WHOQOL-BREF are presented in Table 2. There was a statistically significant improvement in the environmental domain from 61.23 ± 18.16 to 70.11 ± 11.08 (15% improvement) in the WG. When comparing groups, the psychological domain in the post-moment was 20% higher in the WG compared to the CG.
|
Domains |
WG (n = 18) |
CG (n = 15) |
||
|
Pre- |
Post- |
Pre- |
Post- |
|
|
Physical |
61.08 ± 9.04 a |
60.91 ± 7.65 a |
57.32 ± 11.08 |
57.16 ±14.25 |
|
Psychological |
64.11 ± 11.57 |
67.92 ± 7.40 A |
58.33 ± 15.16 |
54.36 ±15.19 A |
|
Social |
70.39 ± 19.76 b |
75.39 ± 13.64 b |
72.49 ± 15.78 |
72.51 ± 34.41 |
|
Environmental |
62.45 ± 17.76 c |
70.45 ± 10.83 c |
64.96 ± 17.92 |
64.02 ± 22.08 |
WG: Water Group; CG: Control Group. Data presented as mean and standard deviation. The same lowercase letters ind
icate statistically significant difference: a (p < 0.0001); b (p = 0.01); c (p = 0.008). When comparing the times when the groups. The same capital letters indicate statistically significant difference: A (p = 0.04) in the comparison between groups in relation to the moments.
Table 3 shows that there was a statistically significant difference in pain domains of 41.83 ± 15.55 to 29.16 ± 14.77 (31% reduction) and physical function of 40.43 ± 13.59 to 32.41 ± 11.54 (20% improvement) in WG.
Table 3 – WOMAC domains
|
Domains |
WG (n = 18) |
CG (n = 15) |
||
|
Pre- |
Post- |
Pre- |
Post- |
|
|
Pain |
40.90 ± 15.17 a |
29.50 ± 14.22 a |
35.52 ± 16.74 |
35.60 ± 16.44 |
|
Stiffness |
43.12 ± 22.38 b |
34.25 ± 20.40 b |
35.37 ± 27.71 d |
42.87 ± 26.94 d |
|
Physical function |
40.04 ± 16.02 c |
32.83 ± 14.52 c |
38.35 ± 18.82 e |
41.12 ± 16.92 e |
WG: Water Group; CG: Control Group. Data presented as mean and standard deviation. The same lowercase letters indicate statistically significant difference: (p = 0.01); b (p = 0.003); c (p = 0.0002); d (p = 0.002); e (p = 0.002) in the comparison between moments in relation to the groups.
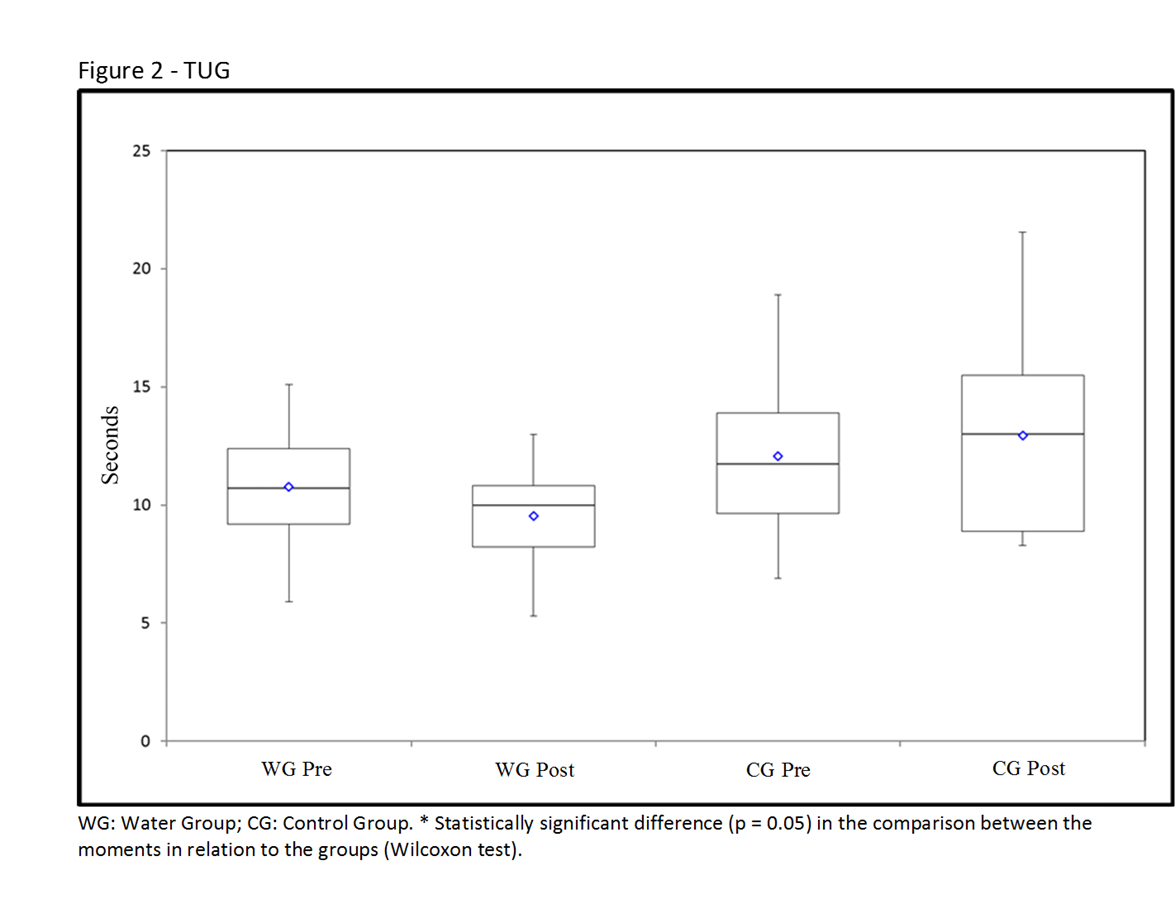
As seen in Figure 2, there was a statistically significant improvement in the TUG test from the WG pre- moment of 10.70 (5.90 to 15.10) seconds to the post- moment of 10.0 (5.30 to 13.0) seconds, with a 6.5% improvement in dynamic equilibrium
Prepared by the authors (2026).
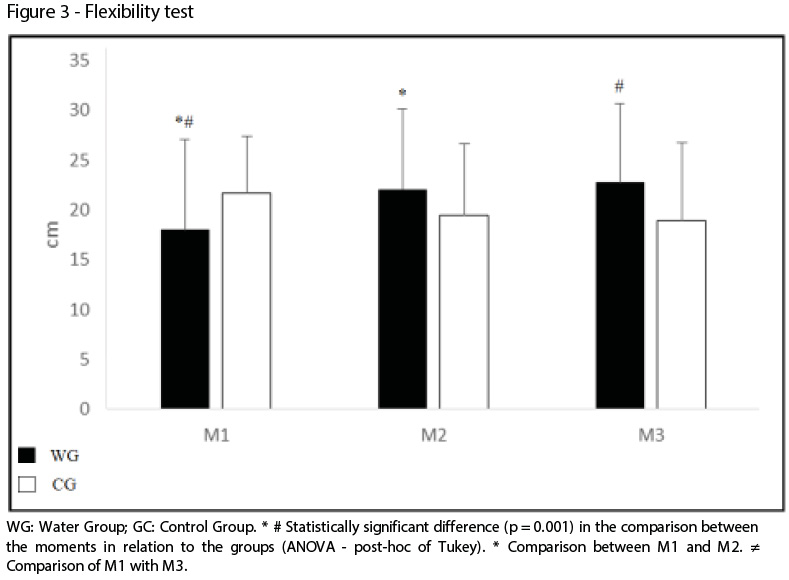
As seen in Figure 3, there was a statistically significant improvement in the increase in flexibility from M1 of 18.0 cm ± 9.13 to M2 of 22.08 ± 8.09 cm (22%) and from M1 to M3 of 22.78 cm ± 7.87 (28%).
Prepared by the authors (2026).
Discussion
This study aimed to investigate the effects of the aquatic physical therapy program on pain intensity, functional ability and quality of life in older adults with knee osteoarthritis. Thus, the method of intervention used promoted a reduction in pain intensity, increased flexibility, improved dynamic balance, physical function and QL.
Aquatic therapy exercises, partial immersion and temperatures between 32° C to 33° C, reduce the joint overload by up to 90%, reducing nociceptive afferents and contributing to the relief of pain [15,16,17,18].
In a systematic review of the literature embracing six studies and containing 800 patients, it was found that functional aquatic exercises promote reduction of pain in elderly patients with knee OA, and is considered a safe and effective alternative therapy in pain control [19].
Aquatic rehabilitation programs in warm water over a minimum of eight weeks and a frequency of three days per week, are effective in the treatment of knee OA, resulting in reduced pain and improved functional ability [20].
With regard to the increase in flexibility, it is believed that the combination of factors such as high water temperature, the thrust and the static stretching exercises of the posterior muscle chain, were responsible for the decrease in painful spasm, facilitating the gain in muscle elasticity and range of joint movement. It should be noted that eight weeks of intervention are sufficient for increased flexibility [21,22,23].
The reduction in the time to execute the TUG test is attributed to the following components of the ATP: motor coordination and agility; balance; space-time perception and reaction speed and muscle training, which biologically contributes to the improvement of neuromuscular activity, proprioception, postural control and functional performance [24].
Studies show that the improvement of functional fitness positively influences the QL of elderly patients with knee OA. This fact concurs with our findings, since there was an improvement in the environmental domain of the WG. By definition, this domain refers to satisfaction in living and social integration [25].
Despite the good results obtained, the experiment showed some methodological limitations. Among them, most importantly, is the lack of standardization of the period of familiarization and adaptation to ATP, as some volunteers had difficulties in understanding and implementing the exercises in the first weeks.
What is highlighted is the excellent structure of the laboratory of therapeutic pools with specific equipment, three levels of depth, an internal and external staircase to aid the displacement of volunteers, non-slip flooring, water temperature maintained at 33° C and the constant supervision provided by the research team. These conditions contributed to the good therapeutic results in an environment that offers ideal conditions for the proper development of the research.
Another important factor is the use of Lequesne’s algofunctional questionnaire as a criterion for inclusion in the study, since the individuals were classified in relation to the physical and functional aspects of daily activities, disregarding the degree of radiological compromise when classifying the severity of OA.
Finally, it is worth mentioning the use of specific and validated assessment tools for individuals with knee OA. In addition, to measure the intensity of pain, we used a dolorimeter with 1 kg precision, ensuring the standardization of pressure application to the four anatomical points on the knee, minimizing subjectivity.
The ATP was based on scientific evidence, with detailed description of the exercises, allowing its easy reproducibility and applicability. It is recommended for elderly patients with knee OA, as it has components that are designed to mitigate pain and to train muscles, thereby promoting increased flexibility, and improved dynamic balance and physical function.
Limitations
Despite the positive findings, this study presents some limitations. The relatively small sample size may limit the generalization of the results to broader populations. Additionally, the absence of long-term follow-up prevents conclusions regarding the maintenance of the therapeutic effects over time. Another limitation was the lack of participant blinding, which may introduce performance bias. Future studies with larger samples, longer follow-up periods, and blinded assessments are recommended.
Conclusion
The aquatic physiotherapy program promoted reduction in pain, an increase and improvement in functional ability and quality of life in elderly patients with knee osteoarthritis.
Ethical Approval
The project was approved by the Research Ethics Committee of the Universidade do Sagrado Coração, opinion number 1,131,248. Before starting the data collection, the participants signed the Free and Informed Consent Term.
Acknowledgements
CAPES (Coordenação de Aperfeiçoamento de Pessoal de Ensino Superior).
Conflicts of interest
None.
Financial support
CAPES (Coordenação de Aperfeiçoamento de Pessoal de Ensino Superior) for financial support.
Authors’ Contributions
Research conception and design: Alcalde GE, Pianna B, Galassi TFB; Data acquisition: Alcalde KGP, Pastor FAC; Data analysis and interpretation: Lopes MF, Chiachio MGE; Manuscript writing: Alcalde GE, Pianna B, Galassi TFB; Critical revision of the manuscript regarding important intellectual content: Arca EA.
References
1. Ginkel AV, Bennell KL, Campbell PK, Wrigley TV, Hunter DJ, Hinman RS. Location of knee pain in medial knee osteoarthritis: patterns and associations with self-reported clinical symptoms. Osteoarthritis Cartilage. 2016;24:1135-1142.
2. Ratzlaff CR, Liang MH. Prevention of injury-related knee osteoarthritis: opportunities for primary and secondary prevention. Arthritis Res Ther. 2010;12:215.
3. Barker AL, Talevski J, Morello RT, Brand CA, Rahmann AE, Urquhart DM. Effectiveness of aquatic exercise for musculoskeletal conditions: a meta-analysis. Arch Phys Med Rehabil. 2014;95:1776-1786.
4. Waller B, Slodownik AO, Vitor M, Lambeck J, Daly D, Kujala UM, Heinonen A. Effect of therapeutic aquatic exercise on symptoms and function associated with lower limb osteoarthritis: systematic review with meta-analysis. Phys Ther. 2014;94:1383-1395.
5. Marx FC, Oliveira LM, Bellini CG, Ribeiro MCC. Tradução e validação cultural do questionário algofuncional de Lequesne para osteoartrite de joelhos e quadris para a língua portuguesa. Rev Bras Reumatol. 2006;46:253-260.
6. Foley A, Halbert J, Hewitt T, Crotty M. Does hydrotherapy improve strength and physical function in patients with osteoarthritis? Ann Rheum Dis. 2003;62:1162-1167.
7. Hollow HS. The Hat [Internet]. Covington; 2012 [cited 2016 Apr 24]. Available from: http://www.harmonyhollow.net/hat.shtml
8. Fleck MPA, Louzada S, Xavier M, Chachamovich E, Vieira G, Santos L, Pinzon V. Application of the Portuguese version of WHOQOL-bref. Rev Saude Publica. 2000;34:178-183.
9. Fernandes MI, Ferraz MB, Ciconelli RM. Tradução e validação do questionário WOMAC para língua portuguesa. Rev Paul Reumatol. 2003;10:25.
10. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC. J Rheumatol. 1988;15:1833-1840.
11. Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP. Validity of four pain intensity rating scales. Pain. 2011;152:2399-2404.
12. Podsiadlo D, Richardson S. The timed “Up & Go”. J Am Geriatr Soc. 1991;39:142-148.
13. Wells KF, Dillon EK. The sit and reach. Res Q Exerc Sport. 1952;23:115-118.
14. Alcalde GE, Fonseca AC, Bôscoa TF, Gonçalves MR, Bernardo GC, Pianna B, Carnavale BF, Gimenes C, Barrile SR, Arca EA. Effect of aquatic physical therapy in older people with knee osteoarthritis. Trials. 2017;18:1-6.
15. Torres-Ronda L, Alcázar XS. The properties of water and their applications for training. J Hum Kinet. 2014;44:237-248.
16. Longpre HS, Maly MR. Identifying exercises appropriate for people with knee osteoarthritis. Osteoarthritis Cartilage. 2014;22:455.
17. Bartels EM, Lund H, Hagen KB, Dagfinrud H, Christensen R, Danneskiold-Samsoe B. Aquatic exercise for knee and hip osteoarthritis. Cochrane Database Syst Rev. 2007;(4):CD005523.
18. Nekouei P, Sadeghi-Demneh E, Mahdavinejad R, Jafarian M. Effects of aquatic exercise on pain and function. Arch Phys Med Rehabil. 2015;96:104-105.
19. Arca EA, Fiorelli A, De Vitta A, Ximenes MA, Gimenes C, Andreo JC. Efetividade do programa de fisioterapia aquática. Rev Kairós Gerontol. 2013;16:73-82.
20. Tacks J, Carpenter MG, Garland SJ, Hunt MA. Factors associated with dynamic balance. Arch Phys Med Rehabil. 2015;96:1873-1879.
21. Gomes-Neto M, Araujo AD, Junqueira IDA, Oliveira D, Brasileiro A, Arcanjo FL. Capacidade funcional e qualidade de vida em idosos com OA. Rev Bras Reumatol. 2016;56:126-130.
22. Kim IS, Chung SH, Park WJ, Kang HY. Effectiveness of an aquarobic exercise program. Appl Nurs Res. 2012;25:181-189.
23. Kluthcovsky ACGC, Kluthcovsky FA. O WHOQOL-bref: revisão sistemática. Rev Psiquiatr. 2009;31:1-12.
