Maria Natália Cardoso1, Rosana Caldas Rêgo de Queiroz1, Douglas Silva Ataíde1, Elorides Brito1, Maíra Mendes dos Santos1, Euler Esteves Ribeiro1, Bruno Mendes Tavares1, Hércules Lázaro Morais Campos1, Elisa Brosina de Leon1
1Universidade Federal do Amazonas (UFAM), Manaus, AM, Brasil
Received: November 18, 2025; Accepted: November 28, 2025.
Correspondence: Maria Natália Cardoso, nataliacardoso301@gmail.com
How to cite
Cardoso MN, Queiroz RCR, Ataíde DS, Brito E, Santos MM, Ribeiro EE, Tavares BM, Campos HLM, Leon EB. Fragility in the organization of health services for old people. Fisioter Bras. 2026;27(1):2953-2966 doi: 10.62827/fb.v27i1.1114
Abstract
Introduction: The aging process increases clinical conditions associated with age, such as urinary incontinence, systemic arterial hypertension, diabetes mellitus, risk of falls, depression, and cognitive decline. There is no consensus on the definition of frailty due to the scope of different physical and biopsychosocial dimensions of the term. Nevertheless, this condition is associated with vulnerability, increasing the chances of falls, functional decline, hospitalization, institutionalization, and death. Objective: Describe and identify clinical/functional dimensions associated with different frailty levels in older people. Methods: A retrospective cross-sectional study was conducted with older adults in Amazonas, Brazil. Variables extracted from the Clinical-Functional Vulnerability Index. The Chi-square test determines the association between the outcome variable and the independent variables. To assess the variables associated with vulnerability, the Poisson model was used. Results: The results show that a total of 497 older people aged 60 to 101 years 216 were classified as robust, 161 pre-frail, and 120 frails. It was concluded that a large part of the older adults in the analyzed community was already in the process of frailty or was fragile. The domains that contributed most to the frailty in each stratum were mood alterations, gait alterations, and deficiency in Activities of Daily Living (basic and instrumental). Conclusion: A large part of the older adults in the analyzed community was already in the process of frailty or was fragile. The domains that most contribute to the frailty in each stratum were mood alterations, gait alterations, and deficiency in activity daily life (basic and instrumental).
Keywords: Aging; Health Services for the Aged; Health of the Elderly; Frailty.
Resumo
Introdução: O processo de envelhecimento aumenta as condições clínicas associadas à idade, como incontinência urinária, hipertensão arterial sistêmica, diabetes mellitus, risco de quedas, depressão e declínio cognitivo. Não há consenso sobre a definição de fragilidade devido à abrangência das diferentes dimensões físicas e biopsicossociais do termo. No entanto, essa condição está associada à vulnerabilidade, aumentando as chances de quedas, declínio funcional, hospitalização, institucionalização e morte. Objetivo: Descreveu-se e identificou-se as dimensões clínico-funcionais associadas a diferentes níveis de fragilidade em idosos. Métodos: Foi realizado um estudo transversal retrospectivo com idosos no Amazonas, Brasil. As variáveis foram extraídas do Índice de Vulnerabilidade Clínico-Funcional. O teste do qui-quadrado determinou a associação entre a variável dependente e as variáveis independentes. Para avaliar as variáveis associadas à vulnerabilidade, utilizou-se o modelo de Poisson. Resultados: Os resultados mostram que, de um total de 497 idosos com idades entre 60 e 101 anos, 216 foram classificados como robustos, 161 como pré-frágeis e 120 como frágeis. Concluiu-se que grande parte dos idosos na comunidade analisada já se encontrava em processo de fragilidade ou era frágil. Os domínios que mais contribuíram para a fragilidade em cada estrato foram alterações de humor, alterações da marcha e deficiência nas Atividades da Vida Diária (básicas e instrumentais). Conclusão: Grande parte dos idosos na comunidade analisada já se encontrava em processo de fragilidade ou era frágil. Os domínios que mais contribuíram para a fragilidade em cada estrato foram alterações de humor, alterações da marcha e deficiência nas atividades da vida diária (básicas e instrumentais).
Palavras-chave: Envelhecimento; Serviços de Saúde para Idosos; Saúde do Idoso; Fragilidade.
Introduction
The world population is aging including Brazil. Seniors aged 65 and over represent 10.49% of the Brazilian population, with a forecast of an increase to 25.17% in 2060 [1]. Aging is a continuous and dynamic process, characterized by chemical and morphological changes. These modifications lead to a loss of harmonic interaction between multiple domains, decreasing the ability to adapt to the environment, and can compromise the health status, increasing the chances of vulnerability [2-4]. This process increases clinical conditions associated with age, such as urinary incontinence, systemic arterial hypertension, diabetes mellitus, risk of falls, depression, and cognitive decline. These health conditions contribute to a greater state of frailty in older people [5,6] requiring the creation of public policies aimed at this population [7].
There is no consensus on the definition of frailty due to the scope of different physical and biopsychosocial dimensions of the term. Nevertheless, this condition is associated with vulnerability, increasing the chances of falls, functional decline, hospitalization, institutionalization, and death [2,3,4,7]. The possibility of intervention addressed to prevent or minimize frailty must be the focus of Health Services addressed for older adults. Some studies demonstrate the possibility of regression of this frailty condition through a multicomponent exercise program, focusing on endurance, strength, coordination, balance, and flexibility improving functional performance [8-10].
Among models traditionally used in geriatric medicine to define this condition, the multidimensional model should be considered a novel approach to including genetic, biological, functional, cognitive, psychological, and socioeconomic dimensions [11]. Several scales assess older adults in a multidimensional way, such as the Clinical-Functional Vulnerability Index-20 (IVCF-20) [2], Edmonton Frail Scale (EFS) [8], and Vulnerable Elders Survey-13 (VES-13) [12]. Different studies use these scales to assess the factors associated with frailty [13,14] or its prevalence in different communities [15], however, it wasn’t found studies that use these scales to elaborate care plans aimed at the needs demonstrated by each level of frailty.
The first step in planning strategies to control and prevent vulnerability in older adults is to carry out a correct functional assessment, allowing for detect risk situations, monitoring functional decline, and identifying areas with greater impairment within the individual assessment of each one and, consequently, identify the need use of specialized services. Knowing the vulnerability of population groups allows us to mobilize personal and physical resources for social transformations, based on intersectoral relationships. Thus, the greater the degree of commitment, resources, scientific quality, monitoring, and management of national, regional, and local social programs for the prevention and care of older people, the greater the chances of directing and optimizing social resources, strengthening the older people in the face of diseases long-term and its consequences.
Therefore, it is necessary to assess the factors that most contribute to frailty among the older community to the elaboration of care plans for each of these strata, aiming to reduce the process of frailty and prevent the evolution of frailty. The understanding of which dimensions greater contribute to each stratum helps health services for the aged to be prepared to create more efficient strategies to help the older people in the community to achieve successful aging. So, the objective of this study was to describe and identify clinical/functional dimensions associated with different frailty levels in older people to help health services deal with frailty.
Methods
Ethical aspects
This project was approved by the Ethics and Research Committee of the Federal University of Amazonas (3,781,478).
Design, place, and period of the study
This is a retrospective cross-sectional study carried out at the Gerontological Polyclinic of the Fundação Universidade Aberta da Terceira Idade (FUnATI) in Manaus, Amazonas/Brazil. The manuscript was written according to The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE).
Population, inclusion, and exclusion criteria
It was a convenience sample, composed of patients aged 60 years or older who reached the Polyclinic for their first assistance from January 2017 to December 2019. Medical records with incorrect completion were excluded. Initially, 744 medical records were collected, and after filtering the final sample consisted of
497 participants
Study protocol
Data collection took place from June to August 2019, through an active search of medical records. Socioeconomic data and the Clinical-functional vulnerability-20 (IVCF-20) were collected by the research team. Double-typing was performed on the overlapping of spreadsheets in the Microsoft Excel® program to check for inconsistencies. In the presence of inconsistency, the medical record number indicated was revised so that the correction could be made. All data were reviewed, tabulated, and coded.
The variables analyzed by the study were based on the dimensions evaluated by the IVCF-20. The instrument is a screening questionnaire composed of 20 questions that assess the older population in the dimensions of age, self-perception of health, activities of daily living (ADL), cognition, mood, mobility, communication, and multiple comorbidities. Based on the score achieved, older people are classified as robust when the score is from 0 to 6; at risk of frailty when the score is between 7 and 14, and frail when it is greater than or equal to 15 [6] (Figure 1).
The purpose of applying the IVCF-20 to the elderly is to identify the specific dimension that contributes to increased vulnerability. The identification of this dimension leads to an individual treatment plan that includes different professionals. Figure 2 demonstrates a proposal of how the dimensions are connected to health areas. For example, an elderly person with impaired mobility, hypertension, and overweight (BMI > 27kg/cm2) should be referred to a physical therapy/occupational therapist, general practitioner/geriatrics, nurse, and nutritionist. If blood pressure is showing acceptable values, the patient can be referred to physical education.
Analysis of results and statistics
Data were grouped and statistically analyzed using the Stata program (version 14.0). A descriptive statistical analysis of the variables studied was performed. The chi-square test was used to assess the association between the outcome variable (vulnerability) and the independent variables. The significance level adopted was 5% (p < 0.05).
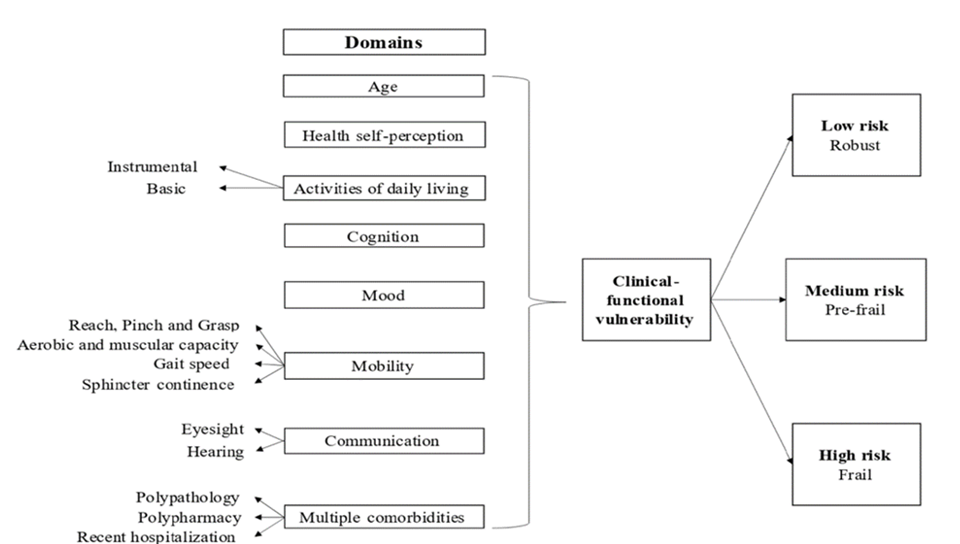
Figure 1 - Multidimensional model components from IVCF-20.
Source: https://www.ivcf20.org/
To assess the variables associated with clinical-functional vulnerability, crude Prevalence Ratios (PR) were first calculated with estimates of 95% confidence intervals (CI) for each variable using the Poisson model. Then, to evaluate the associations of interest, the Poisson multiple regression model with robust variance was applied to calculate the adjusted PR. For this, the variables that presented a p-value lower than 0.20 in the univariate analysis were included, and those that presented statistical significance (p<0.05), when adjusted for the other variables, remained in the final model.
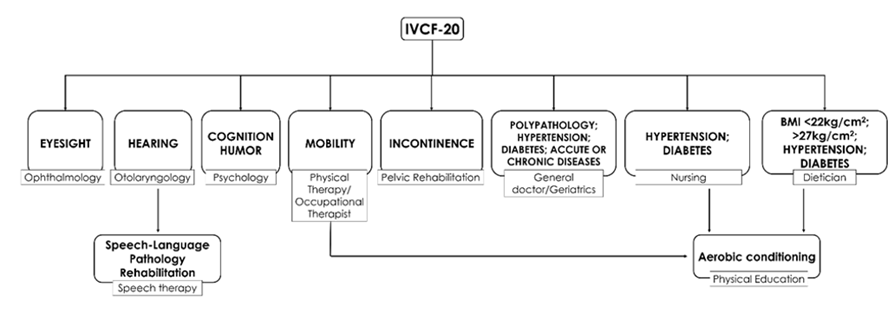
Figure 2 - Proposal flow model based on IVCF-20.
Source: Leon e cols, 2023.
Results
The study included 497 older adults, 69.4% female (n = 345), aged 60 to 101 years (average 69.082 ± 7.77 years). Frailty analysis showed that 43.5% (n = 216) of the older people were classified as robust, 32.4% (n = 161) as pre-frails, and 24.1% (n = 120) were evaluated as frails. Overall, bad/regular health self-perception was assumed by 60.4% (n = 300) of the participants. The majority didn’t report ADL disabilities (the ability to take a shower by themselves). Cognition and mood issues were reported by 48.3% (n = 240) and 59.2%, (n = 294) respectively. A greater number of participants didn’t report mobility alterations, communications difficulties, or the presence of multiple comorbidities (Table 1).
Frail people were older (>85year) and reported bad health self-perception mostly. Also, they presented a major frequency of disabilities and/or difficulties in all other dimensions evaluated: instrumental ADL, basic ADL, cognition alteration, mood alteration, alteration in reach, pinch, and grasp, alteration in aerobic and muscular capacity, gait difficulty, two or more falls in the last month, communication difficulty, and major presence of multiple comorbidities. The older people at risk of frailty showed a worse self-perception of health compared to the robust ones. Both cognition alteration and mood alteration were more present among the frail and at risk of frailty.
Table 1 - Association of IVCF -20* domains with the risk of vulnerability older people treated at the Gerontological Polyclinic. Manaus/AM, from 2017 to 2019 (n = 497).
|
Domain (n; %) |
Total (497, 100%) |
Robust (216; 43.5%) |
Pre-frail (161; 32.4%) |
Frail (120; 24.1%) |
p-value |
|
Sex |
|||||
|
Male |
152 (30.6%) |
63 (29.2%) |
49 (30.4%) |
40 (33.3%) |
0.70 |
|
Female |
345 (69.4%) |
153 (70.8%) |
112 (69.6%) |
80 (66.7%) |
|
|
Age group |
|||||
|
٦٠-٧٤ |
389 (78.3%) |
196 (90.7%) |
129 (80.1%) |
64 (53.3%) |
<0.0001 |
|
٧٥-٨٤ |
83 (16.7%) |
18 (8.3%) |
27 (16.8%) |
38 (31.7%) |
|
|
≥٨٥ |
25 (5%) |
2 (0.9%) |
5 (3.1%) |
18 (15%) |
|
|
Student |
|||||
|
Yes |
254 (51.1%) |
142 (65.8%) |
86 (53.4%) |
26 (21.7%) |
<0.0001 |
|
No |
241 (48.5%) |
73 (33.8%) |
75 (46.6%) |
93 (77.5%) |
|
|
Did not inform |
2 (0.40%) |
1 (0.46%) |
0 (0%) |
1 (0.83%) |
|
|
Health self-perception |
|||||
|
Great, good |
193 (38.8%) |
129 (59.7%) |
47 (29.2%) |
17 (14.2%) |
<0.0001 |
|
Bad, regular |
300 (60.4%) |
85 (39.4%) |
114 (70.8) |
101 (84.2%) |
|
|
Did not inform |
4 (0.80%) |
2 (0.9%) |
0 (0%) |
2 (1.6%) |
|
|
Activities of daily living |
|||||
|
Deficiency in instrumental ADL† |
|||||
|
Yes |
140 (28.2%) |
0 (0%) |
30 (18.6%) |
110 (91.7%) |
<0.0001 |
|
No |
357 (71.8%) |
216 (100%) |
131 (81.4%) |
10 (8.3%) |
|
|
Deficiency in basic ADL† |
|||||
|
Yes |
44 (8.9%) |
0 (0%) |
0 (0%) |
44 (36.7%) |
<0.0001 |
|
No |
453 (91.1%) |
216 (100%) |
161(100%) |
76 (63.3%) |
|
|
Cognition alteration |
|||||
|
Yes |
240 (48.3%) |
58 (26.9%) |
97 (60.3%) |
85 (70.8%) |
<0.0001 |
|
No |
257 (51.7%) |
158 (73.1%) |
64 (39.7%) |
35 (29.2%) |
|
|
Mood alteration |
|||||
|
Yes |
294 (59.2%) |
66 (30.6%) |
124 (77%) |
104 (86,7%) |
<0.0001 |
|
No |
203 (40.8%) |
150 (69.4%) |
37 (23%) |
16 (13.3%) |
|
|
Mobility |
|||||
|
Alteration in Reach, Pinch, and Grasp |
|||||
|
Yes |
47 (9.5%) |
4 (1.9%) |
12 (7.5%) |
31 (25.8%) |
<0.0001 |
|
No |
450 (90.5%) |
212 (98.1%) |
149 (92.5%) |
89 (74.2%) |
|
|
Alteration in aerobic and muscular capacity |
|||||
|
Yes |
153 (30.8%) |
26 (12%) |
55 (34.2%) |
72 (60%) |
<0.0001 |
|
No |
344 (69.2%) |
190 (88%) |
106 (65.8%) |
48 (40%) |
|
|
Gait difficulty |
|||||
|
Yes |
184 (37%) |
15 (6.9%) |
70 (43.5%) |
99 (82.5%) |
<0.0001 |
|
No |
313 (63%) |
201 (93.1%) |
91 (56.5%) |
21 (17.5%) |
|
|
Two or more falls in the last month |
|||||
|
Yes |
78 (15.7%) |
12 (5.6%) |
30 (18.6%) |
36 (30%) |
<0.0001 |
|
No |
413 (83.1%) |
203 (94%) |
128 (79.5%) |
82 (68.3%) |
|
|
Did not inform |
6 (1.2%) |
1 (0.46%) |
3 (1.9%) |
2 (1.7%) |
|
|
Sphincter incontinence |
|||||
|
Yes |
152 (30.6%) |
33 (15.3%) |
68 (42.2%) |
51 (42.5%) |
<0.0001 |
|
No |
345 (69.4%) |
183 (84.7%) |
93 (57.8%) |
69 (57.5%) |
|
|
Communication difficulty |
|||||
|
Yes |
183 (36.8%) |
40 (18.5%) |
68 (42.2%) |
75 (62.5%) |
<0.0001 |
|
No |
314 (63.2%) |
176 (81.5%) |
93 (57.8%) |
45 (37.5%) |
|
|
Presence of multiple comorbidities |
|||||
|
Yes |
134 (27%) |
17 (7.9%) |
45 (28%) |
72 (60%) |
<0.0001 |
|
No |
363 (73%) |
199 (92.1%) |
116 (72%) |
48 (40%) |
|
Note:
* IVCF-20- Clinical Functional Vulnerability Index 20
† ADL – Activities of daily living
Source: Primary data obtained through IVCF-20.
By the adjusted multivariate analysis, the variables associated with robustness were mood alteration and gait difficulty. The variable most associated with those at risk of frailty was a deficiency in basic ADLs and mood changes. The variable most associated with the frail was the deficiency in instrumental ADLs (Table 2). Independently of the stratum of frailty, the most dimensions presented in this sample were mobility/daily living and cognition/mood.
Table 2 - Poisson multiple regression model: variables associated with clinical-functional vulnerability in community-dwelling elderly. Manaus/AM, from 2017 to 2019.
|
Variable (N = 497) |
Crude PR* |
CI† (95%) |
Adjusted PR |
CI (95%) |
|
Robust |
||||
|
Student |
1.18 |
(1.02 – 1.36) |
1.00 |
(0.86 – 1.17) |
|
Age |
1.21 |
(1.03 – 1.42) |
1.03 |
(0.86 – 1.23) |
|
Health self-perception |
1.28 |
(1.11 – 1.49) |
1.08 |
(0.92 – 1.27) |
|
Activities of daily living |
||||
|
Instrumental |
1.43 |
(1.24 – 1.66) |
1.18 |
(0.96 – 1.41) |
|
Basic |
1.31 |
(1.05 – 1.64) |
0.96 |
(0.75 – 1.23) |
|
Cognition |
1.27 |
(1.10 – 1.46) |
1.10 |
(0.95 – 1.28) |
|
Mood |
1.41 |
(1.21 – 1.64) |
1.32 |
(1.13 – 1.54) |
|
Mobility |
||||
|
Reach, Pinch and Grasp |
1.25 |
(1.01 – 1.56) |
1.00 |
(0.79 – 1.27) |
|
Aerobic and muscular capacity |
1.26 |
(1.09 – 1.46) |
1.11 |
(0.95 – 1.28) |
|
Gait |
1.43 |
(1.24 – 1.64) |
1.35 |
(1.17 – 1.56) |
|
Sphincter continence |
1.21 |
(1.05 – 1.41) |
1.10 |
(0.94 – 1.28) |
|
Communication |
1.24 |
(1.07 – 1.43) |
1.08 |
(0.93 – 1.26) |
|
Multiple comorbidities |
1.29 |
(1.11 – 1.50) |
1.14 |
(0.97 – 1.34) |
|
Pre-frail |
||||
|
Student |
1.02 |
(0.89 – 1.16) |
- |
- |
|
Age |
1.02 |
(0.87 – 1.20) |
- |
- |
|
Health self-perception |
0.92 |
(0.80 – 1.06) |
- |
- |
|
Activities of daily living |
||||
|
Instrumental |
1.09 |
(0.94 – 1.27) |
- |
- |
|
Basic |
1.22 |
(0.98 – 1.52) |
1.30 |
(1.03 – 1.63) |
|
Cognition |
0.91 |
(0.76 – 1.04) |
0.94 |
(0.81 – 1.08) |
|
Mood |
0.87 |
(0.76 – 1.00) |
0.84 |
(0.73 – 0.97) |
|
Mobility |
||||
|
Reach, Pinch and Grasp |
1.05 |
(0.83 – 1.31) |
- |
- |
|
Aerobic and muscular capacity |
0.97 |
(0.84 – 1.12) |
- |
- |
|
Gait |
0.92 |
(0.80 – 1.05) |
- |
- |
|
Sphincter continence |
0.90 |
(0.77 – 1.04) |
0.92 |
(0.79 – 1.07) |
|
Communication |
0.96 |
(0.83 – 1.10) |
- |
- |
|
Multiple comorbidities |
0.99 |
(0.85 – 1.15) |
- |
- |
|
Frail |
||||
|
Student |
0.85 |
(0.74 – 0.97) |
0.96 |
(0.83 – 1.11) |
|
Age |
0.81 |
(0.68 – 0.96) |
0.95 |
(0.80 – 1.15) |
|
Health self-perception |
0.87 |
(0.76 – 1.00) |
0.98 |
(0.85 – 1.12) |
|
Activities of daily living |
0.96 |
(0.81 – 1.14) |
||
|
Instrumental |
0.62 |
(0.52 – 0.73) |
0.62 |
(0.52 – 0.73) |
|
Basic |
0.55 |
(0.40 – 0.74) |
0.77 |
(0.54 – 1.08) |
|
Cognition |
0.88 |
(0.77 – 1.01) |
0.95 |
(0.83 – 1.09) |
|
Mood |
0.86 |
(0.75 – 0.98) |
0.97 |
(0.84 – 1.11) |
|
Mobility |
||||
|
Reach, Pinch and Grasp |
0.74 |
(0.58 – 0.96) |
0.94 |
(0.72 – 1.22) |
|
Aerobic and muscular capacity |
0.82 |
(0.71 – 0.95) |
0.96 |
(0.82 – 1.13) |
|
Gait |
0.78 |
(0.68 – 0.90) |
0.95 |
(0.81 – 1.10) |
|
Sphincter continence |
0.92 |
(0.80 – 1.07) |
- |
- |
|
Communication |
0.86 |
(0.74 – 0.99) |
0.93 |
(0.80 – 1.07) |
|
Multiple comorbidities |
0.78 |
(0.69 – 0.92) |
0.90 |
(0.76 – 1.07) |
Note:
* PR - Prevalence Ratios
† CI - Confidence Intervals
Source: Primary data obtained through IVCF-20.
Discussion
Mood/cognition and physical disabilities were the dimensions most associated with frailty in the older people community. Briefly, mood and gait alterations were associated with a low risk of frailty, deficiency in basic ADLs and mood alteration with medium risk, and deficiency in instrumental ADLs with a higher risk of frailty. The presence of these two dimensions highlights the importance of Cognitive-Behavioral Rehabilitation (Psychology) and Physical Rehabilitation. These health areas must be fully integrated and organized into services aimed at assisting older people.
Depression is associated with a higher risk of morbidity and mortality [16]. Patients with depressive symptoms demonstrate symptoms of anxiety, suicidal thoughts, decreased cognitive function, and functional capacity [4,10]. In depressed older subjects, frailty is associated with psychological factors such as the intensity of depressive symptoms [17]. Healthy habits of living, such as practicing physical activities and having a balanced diet, correlate to fewer depressive symptoms among older adults [11,12]. Another factor that can influence these symptoms is remaining working, as it creates a sense of autonomy and independence [1] and enables social interaction [18]. In addition, to cognition being linked to learning, it is also related to the functions of memory, thinking, planning, and reasoning skills [19].
Several studies have linked the impairment of ADLs to frailty [3,7,20,21,22,14] increasing the risk of functional disability in an individual and thus preventing him from living independently and autonomously [5,23]. This corroborates the findings of this study, in which the impairment of basic and instrumental ADLs were the dimensions associated with the groups at risk of frailty and frailness, respectively. Gait speed is a possible indicator of frailty among older adults, through which it is possible to assess the functional and health status of an older person [2,24]. A change in this variable can be a predictor of falls and subsequent decline in the functionality of the aged [25], progressing to hospital admissions and death [6,24,26].
As the profile of the population has already been identified, it is possible to propose strategies that will best accommodate the public in each stratum. As an example of mood alteration, which was more associated with two groups, robust and pre-frail, it is necessary to create a psychological service aimed at this public, in a way that does not interfere with the individual needs of the public that attends the polyclinic. The moment the older adult is classified through the IVCF-20 as being robust or pre-frail, they should be referred to a psychology professional. Even if they don’t demonstrate signs of mood alteration, they are inserted in the groups that demonstrated to have an association with this variable. Another way to address this would be walking sessions, so they should be referred to professionals in physical education as well. There is a correlation between 30-minute walks in active older adults and positive changes in the mood of active older adults [9].
Therefore, not only the psychology service should be activated, but other areas of care can also influence the mood of the patient, demonstrating that the care for the frail should have a multidimensional approach. That can also be seen with cognition and ADLs, as cognition alteration affects the capability of performing these ADLs, and it would be primarily assessed by psychology. But as seen in the literature, a combined cognitive and physical exercise training on cognitive function has shown a positive response in older adults [14], so it would be beneficial to these people if there was an approach combining the services of psychology and physiotherapy/physical education.
The convenience sample in a community center for older adults prevents the results from being generalized, however, the number reached allows statistical inferences to be made about this population. Despite the limitations of the research, it contributes to the elaboration of public policies aimed at each stratum analyzed, reducing the evolution of the frailty process, preventing the evolution to more advanced strata, and regressing the frailty condition. Also, this study provides data support to help health services to improve their structural capacity to better attend to the aging population.
Conclusion
A large part of the older adults in the analyzed community was already in the process of frailty or was fragile. The domains that most contribute to the frailty in each stratum were mood alterations, gait alterations, and deficiency in ADLs (basic and instrumental). For health services to be prepared to deal with frailty, services related to cognitive rehabilitation and physical rehabilitation must be in wide operation.
Conflicts of Interest
The authors declare no conflict of interest.
Funding
This work was financially supported by the Fundação de Amparo à Pesquisa do Amazonas (FAPEAM) and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES 001).
Authors’ contribution
Research conception and design: Leon EB; Data acquisition: Queiroz RCR, Cardoso MN; Data analysis and interpretation: Tavares BM, Queiroz RCR, Santos MM; Manuscript writing: Queiroz RCR; Manuscript revision for important intellectual content: Campos HLM, Leon EB, Brito E, Ribeiro EE, Ataíde DS.
References
1. Amorim JSC, Salla S, Trela CS. Factors associated with work ability in the elderly: systematic review. Rev Bras Epidemiol. 2014;17(4):830–41.
2. Binotto MA, Lenardt MH, Rodríguez-Martínez M del C. Fragilidade física e velocidade da marcha em idosos da comunidade: uma revisão sistemática. Rev Esc Enferm USP. 2018;52:13.
3. Cabral JF, et al. Vulnerabilidade e fatores associados em idosos atendidos pela Estratégia Saúde da Família. Ciênc Saúde Coletiva. 2019;24(9):3227–36.
4. Canêdo AC, Lopes CS, Lourenço RA. Prevalence of and factors associated with successful aging in Brazilian older adults: Frailty in Brazilian older people Study (FIBRA RJ). Geriatr Gerontol Int. 2018;18(8):1280–5.
5. Cruz RR, Beltrame V, Dallacosta FM. Aging and vulnerability: an analysis of 1,062 elderly persons. Rev Bras Geriatr Gerontol. 2019;22(3).
6. De Moraes EN, Silva TM, Oliveira AC, Santos JF, Lima RP, Souza CD. Clinical-Functional Vulnerability Index-20 (IVCF-20): Rapid recognition of frail older adults. Rev Saude Publica. 2016;50:81.
7. Duarte YAO, Lebrão ML, Laurenti R, Menezes TN, Guerra HL, Figueiredo RC, et al. Fragilidade em idosos no município de São Paulo: prevalência e fatores associados. Rev Bras Epidemiol. 2018;21(suppl 2).
8. Fabrício-Wehbe SCC, Schiaveto FV, Vendrusculo TR, Haas VJ, Diefenthaeler F. Cross-cultural adaptation and validity of the “Edmonton Frail Scale - EFS” in a Brazilian elderly sample. Rev Latino-Am Enfermagem. 2009;17(6):1043–9.
9. Geraldes AAR, Ribeiro C, Santos LM, Carvalho AS, Lima RC, Martins RA. Effects of walking on the mood of physically active older people. Rev Bras Med Esporte. 2019;25(1):63–6.
10. Grabovich A, Reynolds CF 3rd, Houck PR, Mazumdar S, Butters MA, Dew MA, et al. Outcomes of subsyndromal depression in older primary care patients. Am J Geriatr Psychiatry. 2010;18(3):227–35.
11. Hertzog C, Kramer AF, Wilson RS, Lindenberger U. Enrichment effects on adult cognitive development. Psychol Sci Public Interest. 2008;9(1):1–65.
12. Maia FOM, Pereira MG, Freitas C, Santos RL, Rocha NS, Castro CM, et al. Adaptação transcultural do Vulnerable Elders Survey-13 (VES-13): contribuindo para a identificação de idosos vulneráveis. Rev Esc Enferm USP. 2012;46(spe):116–22.
13. Instituto Brasileiro de Geografia e Estatística - IBGE. Projeção da população do Brasil e das unidades da federação. Available from: https://www.ibge.gov.br/apps/populacao/projecao/index.html?utm_source=portal&utm_medium=popclock. Accessed 2022 Mar 9.
14. Sousa CR, Lima AC, Oliveira F, Santos RG, Ribeiro EG, Nascimento VM, et al. Factors associated with vulnerability and fragility in the elderly: a cross-sectional study. Rev Bras Enferm. 2022;75(2).
15. Melo Filho J, Oliveira D, Santos I, Freitas R, Pereira L, Nascimento S, et al. Frailty prevalence and related factors in older adults from southern Brazil: A cross-sectional observational study. Clinics. 2020;75:e1694.
16. Ribeiro MCM, Oliveira BR, Santos AV, Lima LM, Costa RS, Nunes FP, et al. Relationship between physical activity and functional capacity change in aged cohort in São Paulo, Brazil. Rev Bras Enferm. 2022;75(3).
17. Oyon J, Lopez-Torres Hidalgo J, Salcedo V, Blasco MA, Martinez-Moreno R, Perez C, et al. Psychosocial factors associated with frailty in the community-dwelling aged population with depression. A cross-sectional study. Aten Primaria. 2021;53(5):102048.
18. Valadares FA, Menezes TN, Silva RV, Souza KM, Oliveira AR, Lima AC, et al. Depressive symptoms can change the lifestyle of the elderly: a cross-sectional case-control study. Motricidade. 2019;15(2–3):52–60.
19. Robertson DA, Savva GM, Kenny RA. Frailty and cognitive impairment—A review of the evidence and causal mechanisms. Ageing Res Rev. 2013;12(4):840–51.
20. Lins MEM, Sampaio RF, Oliveira KA, Pereira MP, Nascimento EF, Gomes SM. Risco de fragilidade em idosos comunitários assistidos na atenção básica de saúde e fatores associados. Saúde Debate. 2019;43(121):520–9.
21. Lourenço RA, Szlejf C, Peixoto SV, Dias RC, Andrade FB, Neri AL, et al. Prevalência e fatores associados à fragilidade em uma amostra de idosos que vivem na comunidade da cidade de Juiz de Fora, Minas Gerais, Brasil: estudo FIBRA-JF. Ciênc Saúde Coletiva. 2019;24(1):35–44.
22. Maia LC, Duarte YAO, Oliveira BR, Rodrigues RA, Nunes BP, Lima-Costa MF, et al.Fragilidade em idosos assistidos por equipes da atenção primária. Ciênc Saúde Coletiva. 2020;25(12):5041–50.
23. Oliveira FMRL, Martins FS, Carvalho JP, Sousa VC, Lima JG, Araújo TS, et al. Frailty syndrome in the elderly: conceptual analysis according to Walker and Avant. Rev Bras Enferm. 2020;73(suppl 3).
24. Ribeiro MCM, Oliveira BR, Santos AV, Lima LM, Costa RS, Nunes FP, et al. Relationship between physical activity and functional capacity change in aged cohort in São Paulo, Brazil. Rev Bras Enferm. 2022;75(3).
25. Silveira T, Dias RC, Lima JC, Santos LP, Oliveira AT, Pereira M, et al. Association of falls, fear of falling, handgrip strength and gait speed with frailty levels in the community elderly. Medicina (Ribeirão Preto). 2015;48(6):549–56.
26. Venturini C, Ferriolli E, de Oliveira DS, Lima NK, Guedes EP, Lobo DS, et al. A multidimensional approach to frailty compared with physical phenotype in older Brazilian adults: data from the FIBRA-BR study. BMC Geriatr. 2021;21(1):246.
